
In this article
Social isolation vs lonelinessHumans: a social animal by biological necessitySocial isolation and toxic relationships: two common biological cascadesA) The immune system shifts into "prolonged alert mode"B) Dysregulation of the stress axis (HPA axis)What distinguishes toxic relationships: unpredictabilityThe neurobiological problem of unpredictabilitySigns that isolation / a toxic relationship is starting to impact your healthClinical signsPotentially affected biological markersOne thing to do this week to reduce biological impactThe essential: make these moments regular and predictable.Why it works biologicallyIf you're in a toxic relationshipIn this article
Social isolation vs lonelinessHumans: a social animal by biological necessitySocial isolation and toxic relationships: two common biological cascadesA) The immune system shifts into "prolonged alert mode"B) Dysregulation of the stress axis (HPA axis)What distinguishes toxic relationships: unpredictabilityThe neurobiological problem of unpredictabilitySigns that isolation / a toxic relationship is starting to impact your healthClinical signsPotentially affected biological markersOne thing to do this week to reduce biological impactThe essential: make these moments regular and predictable.Why it works biologicallyIf you're in a toxic relationship
Love and social connection are therapeutic: Part 1
How your relationships modify your biology, hormones, and longevityFebruary 4, 2026The quality of our relationships, those that support us, those that drain us, those that connect us or isolate us, directly modifies your biology and accelerates or slows down your aging.
The data is clear: in large-scale studies involving over 2 million participants followed for several decades, social isolation and loneliness are both associated with a significant increase in all-cause mortality risk.
Many of us experienced this very concretely during the pandemic: isolation can impact sleep, anxiety, motivation, recovery, and the sense of inner security, sometimes within just a few weeks.
Toxic relationships can maintain chronic stress activation, promote low-grade inflammation, dysregulate cortisol, and weaken sleep. Conversely, stable and secure connections are associated with more favorable trajectories: blood pressure, perceived stress, HRV, recovery, protective behaviors.
Longitudinal studies among the longest in the world place relationship quality at the forefront of long-term health, particularly through its lasting effects on stress, habits, emotional regulation, and protective behaviors.
In this edition, we'll decode these mechanisms and how they become visible and measurable in your biomarkers, physiological signals, and aging trajectories.
Because love is not just an emotion. It's a longevity lever.
And we'll show you how it works and how to measure it.
Social isolation vs loneliness
Social isolation: a measurable fact (few interactions, reduced network, little available support).
Loneliness: a subjective feeling (feeling alone, even when surrounded).
Both matter, but biologically they don't "signal" exactly the same thing: social isolation often implies an objective decrease in protection (help, care, co-regulation, concrete support), which can reinforce physiological burden and translate differently in your biology.
Humans: a social animal by biological necessity
Throughout most of our evolutionary history, survival was not based solely on individual strength, but on group security: access to resources, protection, cooperation, care in case of injury or illness, collective regulation in the face of threats.
This reality shaped our biology. Our nervous, endocrine, and immune systems do not function "in isolation": they are calibrated to interpret social connection as a safety signal, and its loss as a vulnerability signal.
Key point: the brain doesn't wait for an objectively "real" danger to trigger a defense response. It relies on a probability of threat. Historically, being isolated meant: less help, less protection, more risks.
Today, even though the environment is materially safer, the biological logic remains the same: less reliable connection = less perceived security = prolonged activation of defense systems.
Social isolation and toxic relationships: two common biological cascades
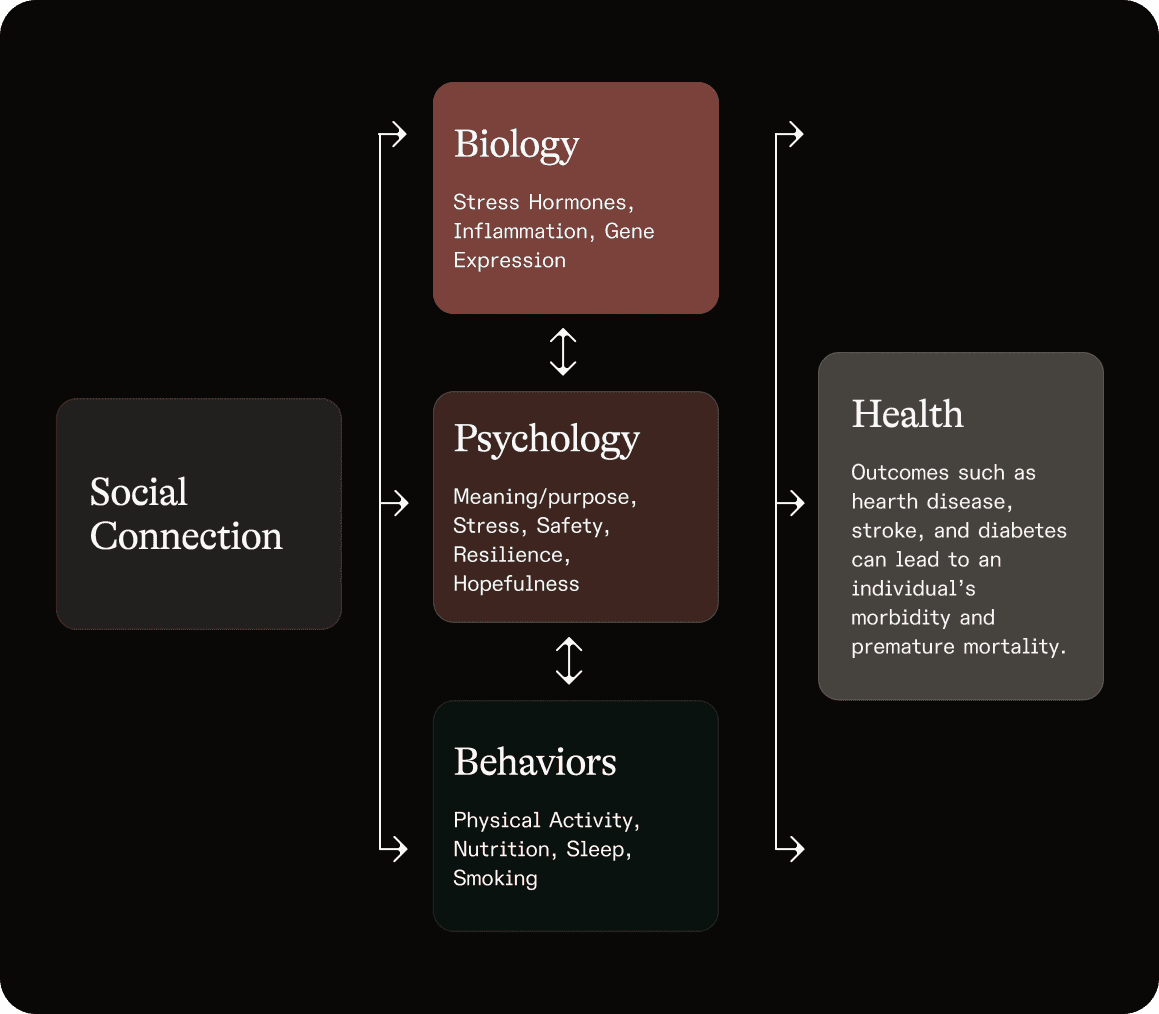
Whether it's social isolation (absence of connection) or toxic relationships (dysfunctional, unpredictable, insecure connection), the brain tends to activate two biological cascades that mutually reinforce each other:
A) The immune system shifts into "prolonged alert mode"
When the brain perceives a less safe social environment, the immune system can profoundly modify its orientation.
What happens concretely:
Your body shifts into survival mode: certain inflammation-related programs activate more, while certain programs related to antiviral defense and adaptive functions are expressed less.
Why this makes sense evolutionarily:
In an ancestral context, social adversity (isolation, rejection, insecurity) could increase the probability of aggression, injury, bacterial infection. An immunity "pre-oriented" toward inflammation/wound healing could therefore be advantageous.
Conversely, exposure to certain respiratory viruses also depends on social contact, which makes plausible a different modulation of antiviral programs depending on context.
The problem today:
If the social insecurity signal becomes chronic, the body can remain stuck in this "prolonged defense" posture.
What this can produce and what Lucis can help you measure:
On inflammation:
Persistent elevation of CRP (C-reactive protein): marker of low-grade inflammation
Imbalance in Omega-3 Index: reflection of your anti-inflammatory capacity
Decrease in vitamin D: essential for immune regulation
On cardiovascular and metabolic health:
Less favorable long-term trajectories, visible in: ApoB (best predictor of cardiovascular risk), lipid profile (LDL-C, HDL-C, Triglycerides), glucose (HbA1c, fasting insulin)
The frequent paradox:
Elevated inflammation (CRP ↑, Omega-3 Index ↓) + less robust antiviral defenses (vitamin D ↓) = your body in "chronic defense mode" depletes its adaptive resources.
B) Dysregulation of the stress axis (HPA axis)
Social isolation or an insecure relational context more easily maintain the brain in hypervigilant mode.
The hormonal cascade
The hypothalamus secretes CRH
The pituitary releases ACTH
The adrenals produce cortisol
Why can cortisol remain "dysregulated"?
In acute stress, cortisol rises then falls. In chronic social stress, it's often a loss of rhythm robustness: the alert signal is reactivated too often, too long, or at the wrong time.
Frequently described profiles:
Less sharp awakening (morning cortisol too low)
Flatter diurnal slope (loss of circadian rhythm)
Less efficient recovery
Possible physiological consequences:
Less favorable insulin sensitivity → visible in: HbA1c, Fasting Insulin, Fasting Glucose
Glycemic variability and cravings (elevated cortisol + disrupted sleep = metabolic imbalance)
Facilitated abdominal storage (hormonal effects + associated behaviors: sleep, snacking, decreased activity)
Modulation of adaptive immunity over time
Neurobiological alterations associated with chronic stress (memory/emotional regulation circuits)
Fragmented sleep: higher evening cortisol + persistent emotional activation = more difficult falling asleep and deep sleep
At Lucis, we help you objectify by measuring:
Cortisol (CAR = Cortisol Awakening Response) your awakening profile that reveals whether your stress axis functions optimally or is dysregulated by chronic stress
DHEA-S (adrenal reserve, often depleted in chronic stress)
HbA1c, Insulin, Glucose (metabolic impact of stress)
Lipids (Triglycerides/HDL often disrupted by chronic stress)
What distinguishes toxic relationships: unpredictability
While isolation and toxic relationships activate common cascades, toxic relationships add a specific dimension: unpredictability, and therefore the impossibility of "deactivating" vigilance.
Large-scale cohort studies show that the perception of "negative aspects" in close relationships (tensions, criticism, excessive demands, repeated conflicts) is associated with a higher risk of coronary events during follow-up.
What is a toxic relationship?
Any relationship where there is permanent conflict, where one seeks to undermine the other, where there is competition, lack of respect, and absence of cohesion.
Possible characteristics:
Asymmetry (one invests, the other withdraws without reciprocity)
Domination/dependence dynamics (self-erasure, cancellation of needs, fear of abandonment)
Dependence (economic, social, emotional, status)
In severe cases: psychological violence, manipulation, coercive control, physical violence.
The neurobiological problem of unpredictability
The brain constantly builds predictive models to conserve energy and maintain security:
In a healthy relationship, the dominant model is: "this person is reliable, I can lower my vigilance"
In a toxic relationship, the system cannot stabilize this model: the interaction can shift without clear signal
Result: sustained vigilance, even during calm phases, because the anticipation of the next "calm" rupture keeps the alert system activated.
Brain networks involved: threat detection, emotional regulation, and social pain networks often described around the amygdala, anterior cingulate cortex, and prefrontal regions (significant inter-individual variability).
Signs that isolation / a toxic relationship is starting to impact your health
Sleep, anxiety, irritability, low motivation, lower HRV, inflammation, cravings, chronic health diseases
Clinical signs
Lighter sleep, nighttime awakenings, difficulty falling asleep "for no reason"
Evening rumination, hypervigilance
Irritability, decreased stress tolerance, emotional fatigue
Sugar cravings (especially late afternoon), "automatic" snacking
Decreased motivation, progressive isolation (self-reinforcing loop)
Diffuse pain / stronger sensation of inflammation
##Physiological" signals (if you track this)
Higher resting heart rate (or "worse recovery")
Lower / more unstable HRV (if measured)
More reactive blood pressure
Erratic energy, "crashes" (often coupled with sleep and blood sugar)
Potentially affected biological markers
hs-CRP / CRP (low-grade inflammation)
fasting glucose / fasting insulin / HbA1c (stress + sleep + behaviors)
lipids (TG/HDL notably)
HPA axis-related markers (Cortisol; DHEA-S)
Biomarkers are not "proof" of a relational problem. But they can be the trace of a system living in defense mode (especially when it "matches" symptoms and trajectory).
One thing to do this week to reduce biological impact
Schedule co-regulation moments during the week
Identify 3 moments in the week where you'll be in synchronous interaction with someone who makes you feel good: phone call, shared walk, coffee, group class, dinner, board game.
The essential: make these moments regular and predictable.
Example:
Monday 6pm: call with a friend
Thursday 12:30pm: lunch with a trusted colleague
Sunday 10am: family breakfast
Put them in your calendar as non-negotiable appointments.
Why it works biologically
Co-regulation is a safety signal: it helps the nervous system come down, promotes oxytocin production, reduces cortisol, supports sleep, decreases rumination, and breaks the loop isolation → stress → fatigue → isolation.
Recurrence is essential: your brain needs repeated and predictable signals.
If you're in a toxic relationship
Prioritize co-regulation moments outside of this relationship. Identify 2-3 people or places where you feel safe, and schedule recurring interactions with them. Your nervous system needs predictable refuges to counterbalance hypervigilance.
In our second edition, we'll explore the other side of the equation: how attachment, co-regulation, and healthy connections activate protective neurochemical cascades. How a 20-second hug modifies your biology. And how to build a "relational ecology" that sustainably supports your health.
This content is provided for informational and educational purposes. It does not replace medical advice, diagnosis, or psychological follow-up.
If you are experiencing violence, or if you do not feel safe, seek help immediately from local emergency services or specialized associations in your country.
REFERENCES
Cole, S. W. (2019). The conserved transcriptional response to adversity. Current Opinion in Behavioral Sciences, 28, 31–37. https://doi.org/10.1016/j.cobeha.2019.01.008
De Vogli, R., Chandola, T., & Marmot, M. G. (2007). Negative aspects of close relationships and heart disease. Archives of Internal Medicine, 167(18), 1951–1957. https://doi.org/10.1001/archinte.167.18.1951
Glass, L. (1995). Toxic People: 10 Ways of Dealing with People Who Make Your Life Miserable. Simon & Schuster.
Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T., & Stephenson, D. (2015). Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspectives on Psychological Science, 10(2), 227–237. https://doi.org/10.1177/1745691614568352
Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social relationships and mortality risk: A meta-analytic review. PLOS Medicine, 7(7), e1000316. https://doi.org/10.1371/journal.pmed.1000316
Kuiper, J. S., Zuidersma, M., Oude Voshaar, R. C., Zuidema, S. U., van den Heuvel, E. R., Stolk, R. P., & Smidt, N. (2015). Social relationships and risk of dementia: A systematic review and meta-analysis of longitudinal cohort studies. Ageing Research Reviews, 22, 39–57. https://doi.org/10.1016/j.arr.2015.04.006
Luo, Y., Hawkley, L. C., Waite, L. J., & Cacioppo, J. T. (2012). Loneliness, health, and mortality in old age: A national longitudinal study. Social Science & Medicine, 74(6), 907–914. https://doi.org/10.1016/j.socscimed.2011.11.028
Marmot, M. G., Smith, G. D., Stansfeld, S., Patel, C., North, F., Head, J., White, I., Brunner, E., & Feeney, A. (1991). Health inequalities among British civil servants: The Whitehall II study. The Lancet, 337(8754), 1387–1393. https://doi.org/10.1016/0140-6736(91)93068-K
Rook, K. S. (2015). Social networks in later life: Weighing positive and negative effects on health and well-being. Current Directions in Psychological Science, 24(1), 45–51. https://doi.org/10.1177/0963721414551364
Shen, C., et al. (2025). Plasma proteomic signatures of social isolation and loneliness. Nature Human Behaviour. Advance online publication. https://doi.org/10.1038/s41562-024-02078-1
Steptoe, A., Shankar, A., Demakakos, P., & Wardle, J. (2013). Social isolation, loneliness, and all-cause mortality in older men and women. Proceedings of the National Academy of Sciences, 110(15), 5797–5801. https://doi.org/10.1073/pnas.1219686110
Valtorta, N. K., Kanaan, M., Gilbody, S., & Hanratty, B. (2018). Loneliness, social isolation and risk of cardiovascular disease in the English Longitudinal Study of Ageing. European Journal of Preventive Cardiology, 25(13), 1387–1396. https://doi.org/10.1177/2047487318792696
Valtorta, N. K., Kanaan, M., Gilbody, S., Ronzi, S., & Hanratty, B. (2016). Loneliness and social isolation as risk factors for coronary heart disease and stroke: Systematic review and meta-analysis of longitudinal observational studies. Heart, 102(13), 1009–1016. https://doi.org/10.1136/heartjnl-2015-308790
Waldinger, R. J., & Schulz, M. S. (2010). What’s love got to do with it? Social functioning, perceived health, and daily happiness in married octogenarians. Psychology and Aging, 25(2), 422–431. https://doi.org/10.1037/a0019087
Waldinger, R. J., & Schulz, M. S. (2023). The Good Life: Lessons from the World’s Longest Scientific Study of Happiness. Simon & Schuster.
Wang, J., Mann, F., Lloyd-Evans, B., Ma, R., & Johnson, S. (2018). Associations between loneliness and perceived social support and outcomes of mental health problems: A systematic review. BMC Psychiatry, 18(1), 156. https://doi.org/10.1186/s12888-018-1736-5
Request an AI summary of Lucis