

Athletic Performance 1/2 : Understanding the Invisible Barriers Holding You Back
What defines or limits your results
Table of contents
Athletic performance. We talk about it constantly. We track it. We measure it in times, watts, reps.
But fundamentally, what makes us perform or conversely, plateau?
Performance isn't just about motivation or training volume.
It's primarily about your biological foundation. About fuel. Oxygen transport. Inflammation. Hormones.
We have created a 2-part series on performance:
In this first edition, we explore what performance really is, and the invisible barriers that limit it.
In the second part, we'll share concrete actions to optimize your biological foundation in measurable ways and gain performance.
The following series will then be dedicated to an inseparable element of performance: recovery.
Let's start by laying the groundwork.
Definition: Athletic Performance
Athletic performance is defined as the capacity to produce optimal physical effort in a given discipline whether endurance, strength, power, or speed.
It's measured objectively:
In time
In load
In aerobic capacity
In anaerobic power
But performing isn't just about running faster or lifting heavier.
It's the sustainable expression of your biological potential without injury, with effective recovery, and while preserving your health.
The Performance Hierarchy
EN - Asset 1_ Sports performance.png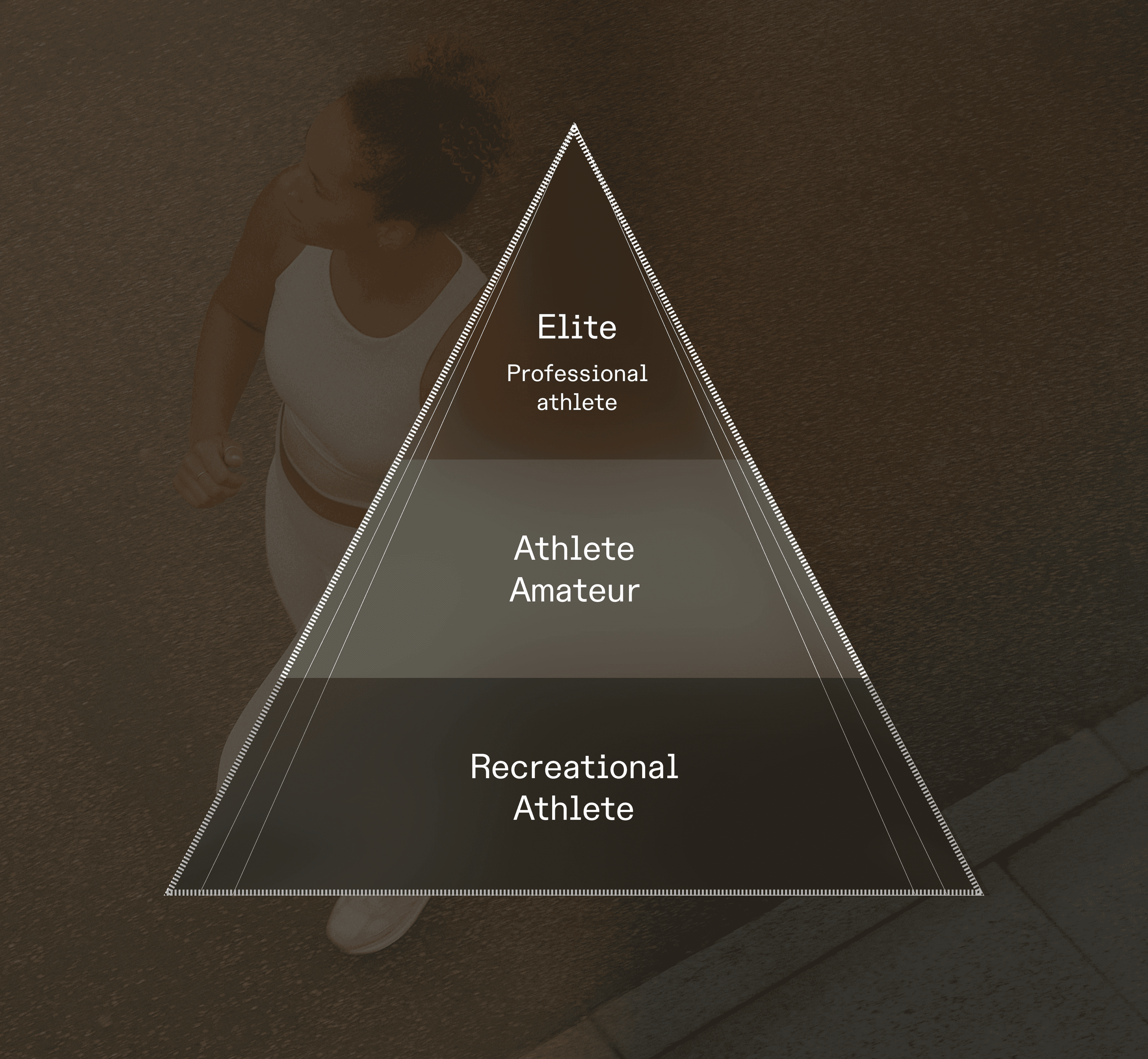
Not everyone who practices a sport trains with the same objectives, volume, or constraints.
Recreational Athlete
Regular practice (2–4 times/week)
Objective: health, well-being, fitness maintenance
Little to no competition
Volume: <6h/week
Amateur Athlete
Structured practice with training plan
Objective: progress, compete
Balance between professional/personal life and sport
Volume: 6–12h/week
Professional / Elite Athlete
Sport is their profession
Objective: podiums, records, medals
Daily medical and nutritional monitoring
Volume: 15–30h/week
This newsletter primarily addresses recreational and amateur athletes. Because they represent the majority of those who practice sport and the most underserved segment. You train seriously. You have goals. You want to progress. But it's not your job, you don't have a medical team, no dedicated nutritionist.
The solution?
Understand what's happening inside your body. Identify invisible biological barriers. And act on them.
The Pillars of Performance: A System, Not a Single Lever
EN - Asset 2_ Sports performance.png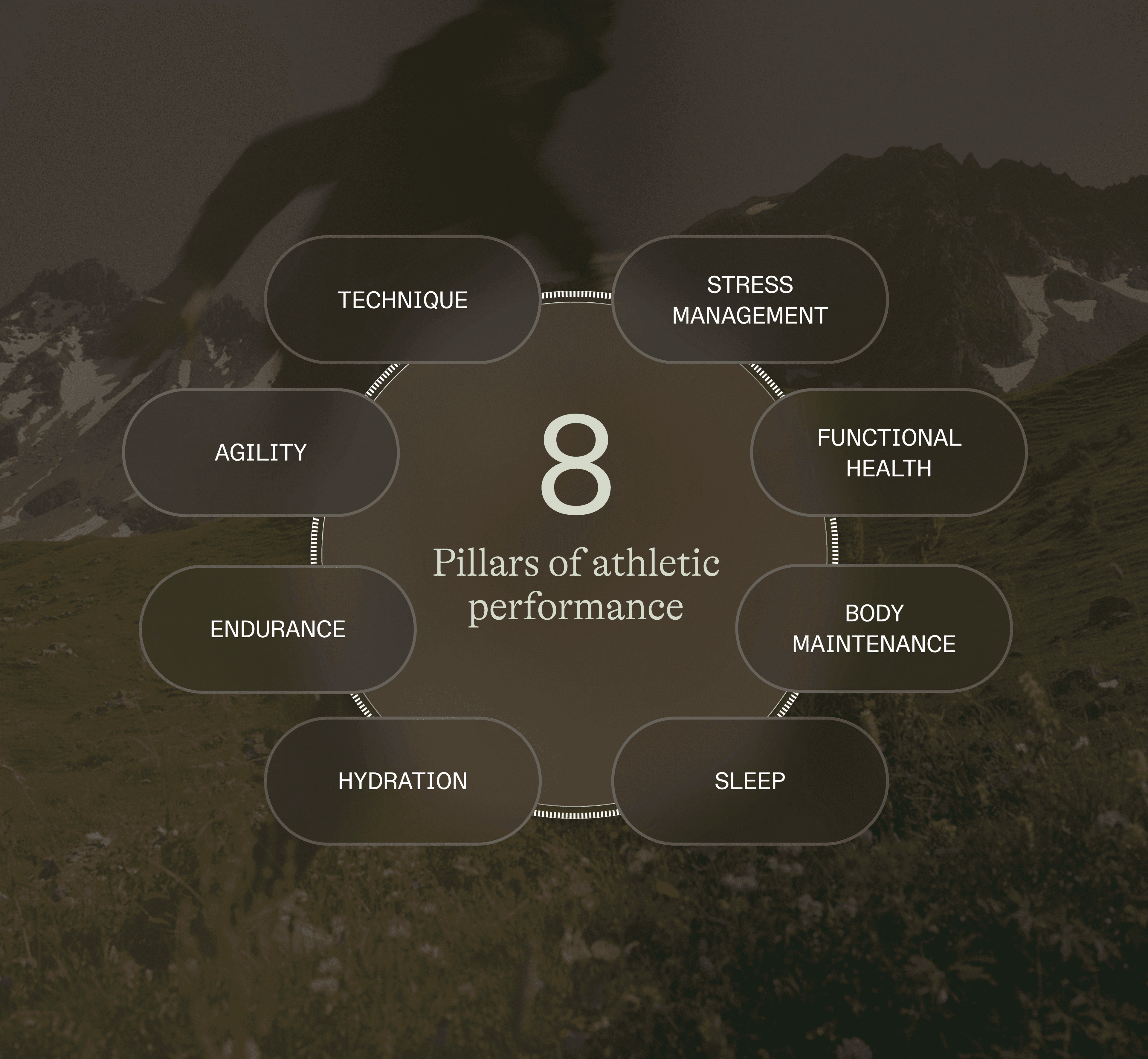
Research in exercise physiology shows that athletic performance is multifactorial.
It depends on both genetic factors (predispositions) and modifiable pillars:
Technique / Sport-specific practice → Movement mastery, repetition, competition
Strength → Muscle development, power
Speed / Agility → Explosiveness, coordination
Endurance / Aerobic capacity → VO₂max, cardiovascular resilience
Nutrition / Hydration → Fuel, timing, food quality
Sleep → Recovery, hormonal adaptation
Body maintenance → Mobility, injury prevention
Functional health / Biomarkers → Biological foundation, hormonal balance
Mental / Stress management → Resilience, motivation, nervous system balance
Many recreational and amateur athletes focus on the most visible pillars: training, nutrition, technique.
But they neglect biological foundation the one that determines your capacity to absorb training, recover effectively, and progress sustainably.
In other words:
You can train perfectly, eat healthily, sleep well and plateau if your functional health (the invisible pillar) has limitations.
3 Invisible Barriers to Performance
Even when training regularly, even when following a structured plan, many recreational and amateur athletes plateau.
Not from lack of willpower. Not from lack of training.
But because their biological foundation has invisible limitations.
Here are the three most common barriers that prevent progression:
1. Oxygen Transport: Ferritin and Hemoglobin
The role: Oxygen is your muscles' primary fuel during effort. It's transported by hemoglobin in red blood cells, and stored as ferritin (iron reserve in the body).
Why it's decisive: If your ferritin or hemoglobin is low, your muscles receive less oxygen. Result: limited aerobic capacity, rapid breathlessness, early fatigue, heavy legs.
Warning signs:
Breathlessness disproportionate to your usual level
Performance that stagnates or regresses despite training
Chronic fatigue, pallor, brittle nails
Difficulty maintaining intensity during long efforts
Scientific data: Ferritin < 30 ng/mL is associated with a significant decrease in aerobic capacity, even without clinical anemia.
Critical point: Women of childbearing age are particularly at risk due to menstrual losses. Up to 15–35% of female athletes have iron deficiency.
Important: Never supplement with iron without a complete prior blood test.
2. Glucose Management: HbA1c and Glycemic Stability
The role: Glucose is one of your fuels during effort, especially at moderate to high intensities. Your capacity to mobilize, store, and use it efficiently determines your energy stability.
Why it's decisive: If your HbA1c (reflection of your average blood glucose over 3 months) is elevated or unstable, it indicates poor glucose management. Result: energy crashes during effort, cravings, slowed recovery, difficulty maintaining intensity.
Warning signs:
Energy crashes after meals or mid-day
Constant need for sugar during training
Rollercoaster energy (spike then crash)
Difficulty sustaining long efforts without carbohydrate intake
The data: An HbA1c > 5.7% may reflect reduced insulin sensitivity, which limits glucose uptake by muscles.
Critical point: Glycemic instability reduces metabolic flexibility the body's ability to alternate between glucose and lipids as energy sources. Result: sugar dependency, rapid fatigue, limited performance on long efforts.
3. Chronic Inflammation: CRP (C-Reactive Protein)
The role: Training induces acute inflammation it's normal, and even necessary. This stress triggers adaptation: your muscles strengthen, your cardiovascular capacity improves.
Why it's decisive: But if your CRP (marker of systemic inflammation) remains elevated chronically, it means your body is suffering the training instead of absorbing it. Result: fatigue accumulation, no progression, increased injury risk.
Warning signs:
Soreness persisting beyond 48–72h
Non-restorative sleep, night awakenings
Irritability, decreased motivation
Feeling "drained" constantly, even after a rest day
The data: Elevated CRP indicates systemic inflammation. For cardiometabolic prevention, we target hs-CRP < 1 mg/L.
Critical point: Chronic inflammation is amplified by:
Sleep deprivation (< 7h/night)
Pro-inflammatory diet (refined sugars, trans fats, alcohol)
Chronic psychological stress
Training overload without adequate recovery
💡 Key Takeaway: Functional Health for Performance
Performance depends on a biological ecosystem. That is, the interaction between your biomarkers, your sleep, your stress management, your micronutrients (vitamin D, magnesium, B12), your hydration, your body composition.
This is what we call functional health applied to performance: Optimizing your biological foundation so that each training session is absorbed, each effort produces an adaptation, and each progress is sustainable.
Clear data, actionable levers, and measurable results.
At Lucis, we help you better understand your biology to improve your athletic performance.
In part 2 we discuss how to take action. We analyze how to concretely optimize the biological pillars of performance with nutrition and lifestyle strategies.
References
Beard, J., & Tobin, B. (2000). Iron status and exercise. The American Journal of Clinical Nutrition, 72(2), 594S-597S.
Brownlie, T., et al. (2004). Marginal iron deficiency without anemia impairs aerobic adaptation among previously untrained women. The American Journal of Clinical Nutrition, 79(3), 437-443.
Deldicque, L., & Francaux, M. (2008). Functional food for exercise performance: fact or foe? Current Opinion in Clinical Nutrition & Metabolic Care, 11(6), 774-781.
Hackney, A. C., & Walz, E. A. (2013). Hormonal adaptation and the stress of exercise training: the role of glucocorticoids. Trends in Sport Sciences, 20(4), 165-171.
Kasapis, C., & Thompson, P. D. (2005). The effects of physical activity on serum C-reactive protein and inflammatory markers: a systematic review. Journal of the American College of Cardiology, 45(10), 1563-1569.
Leproult, R., & Van Cauter, E. (2011). Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA, 305(21), 2173-2174.
McClung, J. P., & Murray-Kolb, L. E. (2013). Iron nutrition and premenopausal women: effects of poor iron status on physical and neuropsychological performance. Annual Review of Nutrition, 33, 271-288.
Meeusen, R., et al. (2013). Prevention, diagnosis, and treatment of the overtraining syndrome: joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Medicine & Science in Sports & Exercise, 45(1), 186-205.
Ridker, P. M. (2003). Clinical application of C-reactive protein for cardiovascular disease detection and prevention. Circulation, 107(3), 363-369.
The information provided is for educational purposes only and does not replace medical advice.
Written by Anaïs Gautron
More insights, straight to your inbox.
New articles on biomarkers, performance, and wellness — no noise, just substance.